It’s important to understand COVID-19; Here’s what we know
Image: Open Source Ventilator, Pakistan; Muhammad Umair
Epidemiology of COVID-19
The COVID-19 pandemic has exploded since the disease was first identified in China in December of 2019. As of July 24, 2020, more than 15 million cases of COVID-19 have been reported globally, including more than 600,000 deaths, across 188 countries and territories (including all 50 states of the United States). It is estimated that approximately 8 million people have recovered.[1] Individuals of all ages are at risk for infection and severe disease. However, the probability of serious complications and fatal disease is highest in people over the age of 65 years and those living in long-term care facilities or nursing homes. Others at particularly high risk for COVID-19 are people of any age with existing underlying conditions, especially when not well-controlled. [2,3]
Transmission of COVID-19
The onset and duration of viral shedding and period of infectiousness are not completely defined. Asymptomatic or pre-symptomatic individuals infected with COVID-19 may have viral RNA detected in upper respiratory specimens before the onset of symptoms.[4] Additionally, transmission from asymptomatic individuals has been described.[5]
The time from exposure to onset of symptoms is typically around five days but may range from two to fourteen days.[6] The virus is primarily spread between people during close contact,[7] often via small droplets produced by coughing, sneezing, or talking.[8] Additionally, these droplets fall to the ground or onto surfaces where people may also become infected by touching a contaminated surface and then touching their face, nose, mouth, or eyes.[9]
Smaller respiratory droplets, known as aerosols, have the ability to remain suspended in air for a longer amount of time and can transmit the virus if they are inhaled by others. There have been reported outbreaks of COVID-19 in closed settings (such as restaurants, bars, and places of worship) where people were shouting, talking, or singing. These likely crowded and poorly ventilated spaces facilitated the spread of infectious aerosols.[10]
It appears that the virus that causes COVID-19 can spread from people to animals in some situations. The USDA previously confirmed COVID-19 infection in one tiger at a zoo in New York after several large cats began to suffer from respiratory illness.[11] The CDC is aware of a small number of pets, including cats and dogs, reported to be infected with the virus that causes COVID-19. These infections occurred after the animals had close contact with people actively infected with COVID-19.[12] Infected pets may show signs of illness or they may not have any symptoms. Of the pets that have been infected, most only had mild illness and fully recovered.[13]
Clinical Presentation of COVID-19
The spectrum of illness from COVID-19 can range from asymptomatic infection to severe pneumonia with acute respiratory distress syndrome (ARDS) and death. In a summary of 72,314 persons with COVID-19 in China, 81% of cases were reported to be mild, 14% were severe, and 5% were critical.[14] Symptoms may appear anywhere from 2-14 days after exposure to the virus. The most common symptoms of COVID-19 include: fever or chills, cough, shortness of breath or difficulty breathing, fatigue, body aches, headache, loss of taste or smell, sore throat, runny nose or congestion, nausea or vomiting, diarrhea.[15]
Common laboratory findings of COVID-19 include leukopenia and lymphopenia. Other laboratory abnormalities have included elevations in aminotransferase levels, C-reactive protein, D-dimer, ferritin, and lactate dehydrogenase.[16] Critically ill patients were found to have elevated inflammatory markers with an increased risk for thrombosis (blood clots) secondary to an increase of inflammatory cytokines and activation of coagulation (clotting) factors.[17]
Abnormalities in chest X-ray vary, but typically reveal bilateral multifocal opacities. Chest x-rays obtained early during the course of infection may not reveal significant changes.[18] Abnormalities seen in computed tomography (CT) of the chest also vary, but typically reveal bilateral peripheral ground-glass opacities with the development of areas of consolidation later in the clinical course.[19]
Diagnosing COVID-19
The diagnosis of a COVID-19 patient requires detection of SARS-CoV-2 RNA by reverse transcription polymerase chain reaction (RT-PCR). Detection of viral RNA is best when collected from nasopharynx samples compared to throat samples. Lower respiratory samples may have better yield than upper respiratory samples.[20,21] The detection of SARS-CoV-2 RNA in blood may be a marker of severe illness.[22]
Viral RNA shedding may persist over longer periods among older persons and those who had severe illness requiring hospitalization.[23] Infection with both SARS-CoV-2 and with other respiratory viruses has been reported, and detection of another respiratory pathogen does not rule out COVID-19.[24]
Antigen tests for SARS-CoV-2 were recently authorized. This new category of tests can detect fragments of proteins from the virus when samples are collected from within the nasal cavity. This type of test was developed for the rapid identification of acute COVID-19 infection and provides faster results than the RT-PCR method.[25] Antibody testing is available to detect a previous infection with COVID-19. Most people will produce antibodies 1-3 weeks after exposure to the virus, but it is unclear how long these antibodies will remain with the person or if any future protection against COVID reinfection is offered.[26]
Treatment of COVID-19
Patients with a mild clinical presentation (without viral pneumonia and hypoxia) may not require hospitalization, and many patients will be able to manage their illness at home. The decision to monitor a patient in the inpatient or outpatient setting should be made on a case-by-case basis.[27] This decision will depend on the clinical presentation, requirement for supportive care, risk factors for complications, and if the patient is able to self-isolate at home. Patients with risk factors for severe illness should be monitored closely given the possible risk of progression to severe illness during the second week following symptom onset.[28,29]
No specific treatment for COVID-19 is currently FDA approved; however, in accordance with preliminary clinical trial data, the COVID-19 Treatment Guidelines Panel (NIH) have recommended the investigational antiviral drug remdesivir for the treatment of COVID-19 in hospitalized patients with severe disease (O2 ≤94% on room air), requiring supplemental oxygen or mechanical ventilation. Remdesivir is not approved by the FDA, and is only available through an FDA emergency use authorization, in clinical trials, or through an emergency access program for children and pregnant patients.[30][31]
While corticosteroids have been widely used in hospitalized patients with severe illness in China [32], the benefit of corticosteroid use cannot be determined based upon uncontrolled observational data. The use of corticosteroids may be indicated for other reasons, such as management of chronic obstructive pulmonary disease or septic shock.[33] The COVID-19 Treatment Guidelines Panel (NIH) recommends using dexamethasone for the treatment of COVID-19 in patients who are mechanically ventilated and in patients who require supplemental oxygen but who are not mechanically ventilated.[34]
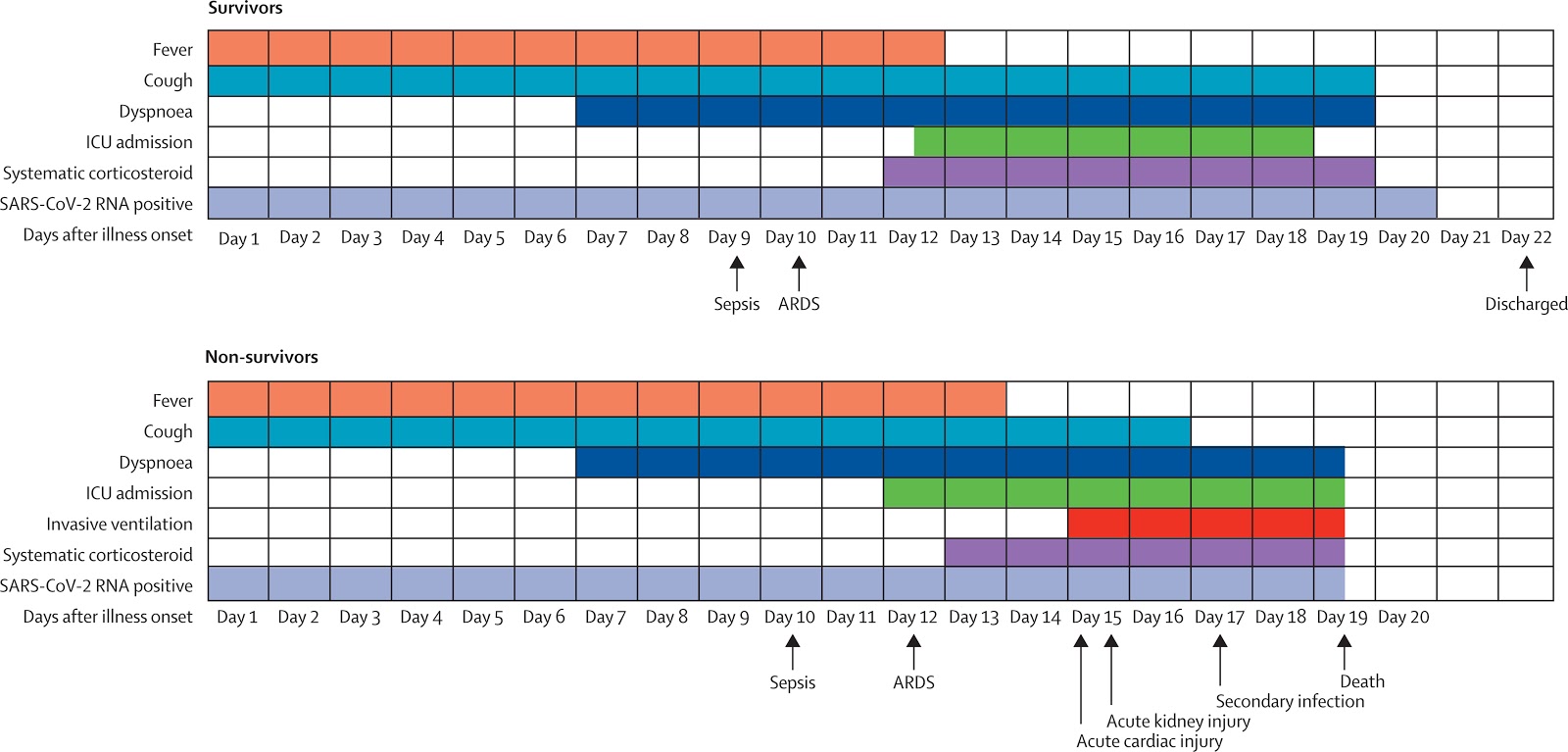
The majority of inpatient management revolves around the supportive management of the most common complications of severe COVID-19: pneumonia, hypoxemic respiratory failure/ARDS, sepsis and septic shock, cardiomyopathy and arrhythmia, acute kidney injury, and complications from prolonged hospitalization including secondary bacterial infections, thromboembolism, gastrointestinal bleeding, and critical illness polyneuropathy/myopathy. [35,36,37,38]
Clinical Resources
Information for Healthcare Professionals about Coronavirus (COVID-19)(CDC)
ADACoronavirus (COVID-19) Center for Dentists (ADA)
Q&A on coronaviruses (COVID-19) (WHO)
Coronavirus Disease 2019 (COVID-19) (FDA)
FEMA Releases Latest State-by-State COVID-19 Data (FEMA)
Visualization of Symptoms of COVID19 Over Time, ~5 Days After Exposure
Take Action
Volunteers from 55+ countries on 6 continents have produced and distributed millions of medical supplies in response to the COVID-19 Pandemic. You can take a part in this effort to fight the virus and slow its spread.

Image: PUC Rio, Rio de Janeiro, Brésil; Marcelo Balisteri